Introduction
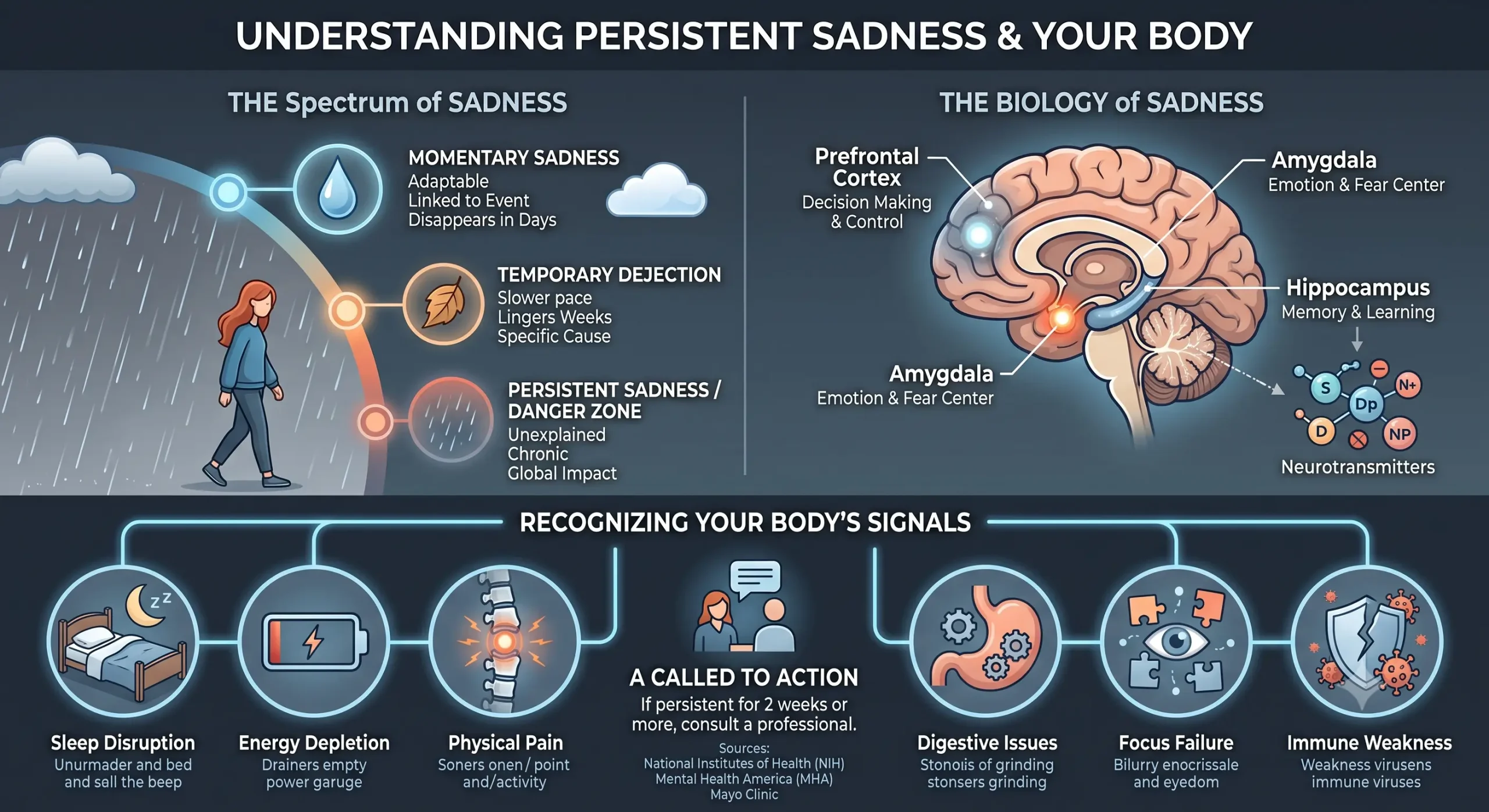
Sadness is a universal and deeply human emotion—a natural response to loss, disappointment, or life’s inevitable challenges. It serves an important adaptive purpose, signaling to ourselves and others that we may need support and prompting us to reflect on what matters . However, when sadness persists for weeks or months, becoming a constant companion that colors every aspect of daily life, it may be signaling something more serious: a depressive disorder that warrants attention and care.
Understanding the difference between normal sadness and clinical depression is essential for protecting your mental health and well-being. This article explores the spectrum of sadness, from typical emotional responses to persistent depressive states, drawing on authoritative medical and research sources to help you recognize what your mind and body may be telling you.
The Crucial Distinction: Normal Sadness vs. Clinical Depression
What Is Normal Sadness?
Sadness is a healthy, normal emotional response to difficult circumstances. It typically has a clear trigger—a relationship ending, the death of a loved one, job loss, or disappointment . Normal sadness tends to:
Come and go in waves, not dominate every moment
Lessen over time as you process the experience
Allow you to experience other emotions alongside the sadness
Not completely disrupt your ability to function at work, in relationships, and in daily activities
As the CDC explains, “Being sad is a normal reaction in difficult times. Usually, the sadness goes away” .
When Sadness Becomes Depression
Clinical depression—also called major depressive disorder or persistent depressive disorder—represents a fundamentally different state. The Mayo Clinic emphasizes that depression “isn’t a weakness or a character flaw. It’s not about being in a bad mood, and people who experience depression can’t just snap out of it” .
The key distinguishing features include:
| Normal Sadness | Clinical Depression |
|---|---|
| Has a clear, identifiable trigger | May have no clear cause or seem disproportionate |
| Temporarily affects mood | Causes persistent symptoms lasting 2 weeks or more |
| Doesn’t significantly impair daily functioning | Interferes with work, relationships, and self-care |
| Allows for moments of relief or positive emotion | Creates a pervasive sense of emptiness or numbness |
| Doesn’t involve physical symptoms | Often includes sleep, appetite, and energy changes |
What Prolonged Sadness May Be Telling You: The Differential Diagnosis
When sadness doesn’t resolve, it can point to several different conditions. Understanding these possibilities is critical, as treatment approaches vary significantly.
1. Major Depressive Disorder (MDD)
MDD is the most commonly recognized form of depression. According to the DSM-5 criteria, diagnosis requires a depressed mood or loss of interest/pleasure (anhedonia) for at least two weeks, accompanied by at least five of the following symptoms:
Significant weight loss or gain, or changes in appetite
Sleep disturbances: insomnia or sleeping too much (hypersomnia)
Psychomotor changes: agitation or slowing of movement
Fatigue or loss of energy nearly every day
Feelings of worthlessness or excessive guilt
Difficulty concentrating or making decisions
Recurrent thoughts of death or suicide
The lifetime incidence of depression in the United States is more than 12% in men and 20% in women, making it one of the most common mental health conditions .
2. Persistent Depressive Disorder (PDD / Dysthymia)
Previously called dysthymia, PDD is characterized by a chronic depressed mood lasting at least two years (one year in children/adolescents). During this time, symptoms are present “more days than not” and don’t remit for more than two months at a time .
Key features include:
Depressed mood most of the day, most days
At least two of: poor appetite/overeating, insomnia/hypersomnia, low energy, low self-esteem, poor concentration, or hopelessness
As the BMJ Best Practice notes, PDD is “frequently misdiagnosed because the correct criteria to diagnose this condition are often not applied” . People with PDD often describe themselves as having “always been this way” and may not recognize their chronic low mood as a treatable condition.
3. Bipolar Disorder (Depressive Phase)
Depression can also occur as part of bipolar disorder. In this condition, depressive episodes alternate with periods of mania or hypomania—characterized by elevated mood, increased energy, reduced need for sleep, and sometimes impulsive behavior. Depressive phases in bipolar disorder can be indistinguishable from MDD, making a thorough history crucial for correct diagnosis .
4. Adjustment Disorder with Depressed Mood
When significant sadness develops in response to an identifiable stressor—such as a serious medical diagnosis, divorce, or financial crisis—it may be an adjustment disorder. Unlike MDD, symptoms:
Occur within 3 months of the stressor
Are out of proportion to the severity of the stressor
Do not meet full criteria for major depression
Often resolve when the stressor is addressed or coping improves
5. Grief
Grief is a normal response to loss, typically lasting 2 to 6 months. Its symptoms include sadness, tearfulness, and insomnia—but unlike depression, grief:
Does not result in low self-esteem or worthlessness
Allows for periods of normal functioning
Usually involves feelings of loss and yearning rather than a pervasive sense of emptiness
However, complicated grief—where symptoms persist, intensify, or include thoughts of suicide—requires professional intervention.
6. Medical Conditions That Can Cause Sadness
Depressed mood can be a symptom of an underlying medical condition, making a medical evaluation essential before assuming a purely psychiatric cause. According to the NIH, conditions linked with sadness include:
Endocrine Disorders:
Hypothyroidism (underactive thyroid): often presents with fatigue, weight gain, cold intolerance, and depressed mood
Cushing’s syndrome (excess cortisol): can cause mood changes, weight gain, and irritability
Neurological Conditions:
Stroke (cerebrovascular accident): depression occurs in 6%–52% of acute stroke patients
Parkinson’s disease: depression often precedes motor symptoms
Multiple sclerosis, brain tumors, dementia
Seizure disorders
Other Medical Conditions:
Cancer (especially pancreatic cancer)
Infectious diseases: influenza, mononucleosis, viral hepatitis
Collagen vascular diseases: lupus, rheumatoid arthritis
Sleep apnea with hypoxia
Chronic pain conditions
Diabetes, heart disease
Medication-Induced Depression:
Certain medications can trigger depressive symptoms, including:
Interferon-alpha (used for hepatitis C and some cancers)
Corticosteroids (prednisone)
Cimetidine, disulfiram
Some beta-blockers and blood pressure medications
7. Demoralization
Demoralization deserves special attention, particularly among those with chronic or serious medical illness. It involves feelings of:
Being unable to cope
Helplessness and hopelessness
Personal failing and aloneness
Despair and disempowerment
Demoralization differs from major depression because mood responsivity is preserved—when circumstances improve, the person can still experience enjoyment and hope. However, it can coexist with depression and requires recognition for appropriate support .
8. Substance/Medication-Induced Depressive Disorder
Alcohol, sedatives, opioids, and stimulants (during withdrawal) can cause persistent depressed mood. A thorough substance use history is essential in evaluation .
Recognizing the Signs: When to Seek Help
Symptoms You Shouldn’t Ignore
The CDC and mental health organizations identify these key warning signs:
Emotional Signs:
Feeling sad, empty, or hopeless often or all the time
Not wanting to do activities that used to be fun (anhedonia)
Feeling irritable, easily frustrated, or restless
Physical Signs:
Unplanned weight change or changes in appetite
Trouble falling asleep or staying asleep, or sleeping too much
Lack of energy or feeling tired constantly
Cognitive Signs:
Trouble concentrating, remembering things, or making decisions
Feeling worthless or excessively guilty
Recurrent thoughts of death or suicide
The Two-Week Threshold
Mental health professionals typically look for symptoms lasting at least two weeks as a marker for potential clinical depression . However, as the CDC advises: “If your symptoms are not going away, getting worse, or affecting your daily activities, make an appointment with a counselor or other mental health professional” .
Immediate Help for Crisis
If you or someone you know is experiencing thoughts of suicide or self-harm:
Call or text 988 (988 Suicide & Crisis Lifeline) for 24/7 support
Or chat with someone at 988lifeline.org
Seek emergency care immediately
Understanding the Causes: A Biopsychosocial Perspective
Biological Factors
Genetics: A family history of depression increases risk—approximately one in six people will experience a major depressive episode in their lifetime
Brain chemistry: Disruptions in neurotransmitters like serotonin, dopamine, and norepinephrine play a key role
Hormonal changes: Pregnancy, menopause, and thyroid disorders
Chronic health conditions: Diabetes, heart disease, and thyroid disorders contribute to depression risk
Social Factors
Traumatic or stressful life events
Limited access to resources such as food, housing, and healthcare
Lack of social support
Isolation and loneliness
Psychological Factors
Negative thinking patterns
Problematic coping behaviors such as avoidance and substance use
Low self-esteem and perfectionism
Chronic stress
Treatment Options: Help Is Available
Medications
Antidepressants—particularly SSRIs (selective serotonin reuptake inhibitors) like sertraline and escitalopram—are effective for many people. Research suggests that medication may have a stronger effect than psychotherapy for persistent depressive disorder, though a combination approach often yields the best results .
Psychotherapy
Several evidence-based therapies are effective:
Cognitive Behavioral Therapy (CBT): Helps identify and restructure negative thinking patterns. Adding CBT to antidepressants more than doubled response rates in patients with treatment-resistant depression
Interpersonal Therapy (IPT): Focuses on current relationship problems and social functioning
Psychodynamic Therapy: Helps develop understanding of relationships and reduce maladaptive interpersonal patterns
Combination Treatment
Research shows the greatest effect when medication and psychotherapy are combined, especially for persistent depression .
Lifestyle Interventions
Regular aerobic exercise 4–6 times per week has been shown to improve depressive symptoms. Maintaining social connections, adequate sleep, and a healthy lifestyle also support recovery .
Duration of Treatment
Because persistent depression is chronic, long-term maintenance is often needed:
Acute phase: 12 weeks of treatment
Continuation phase: 6 months of continued treatment
Maintenance: At least one year for those with a history of two or more episodes, and sometimes lifelong for those with frequent relapses or severe illness
Expert Sources and Resources
This article draws on authoritative medical and research sources. For further reading:
Leading Medical Organizations
Mayo Clinic – Comprehensive depression information and treatment guidance
Centers for Disease Control and Prevention (CDC) – Public health guidance on sadness and depression
World Health Organization (WHO) – Global perspectives and resources on depression
National Institutes of Health (NIH) / PubMed Central – Peer-reviewed research articles on depression and related conditions
Clinical Diagnostic Resources
BMJ Best Practice: Persistent Depressive Disorder – Evidence-based clinical guidelines (subscription may be required)
Medscape: Dysthymic Disorder Treatment – Clinical overview and treatment approaches
Psychiatric Times: PDD Update – In-depth discussion of diagnosis and treatment
Crisis Support
988 Suicide & Crisis Lifeline – Free, confidential crisis support 24/7
Conclusion
Sadness is part of being human, but when it doesn’t go away, it’s not a sign of weakness—it’s a signal that you may need support. Whether the cause is a life stressor, a treatable mood disorder, or an underlying medical condition, help is available.
The most important step is reaching out. As the CDC reminds us: “Depression is not your fault. Getting support helps you and your loved ones” .
You don’t have to navigate this alone. Talk to a healthcare provider, reach out to a trusted friend, or contact a crisis line. Understanding what your mind and body are telling you is the first step toward getting the care you deserve.
