Abstract
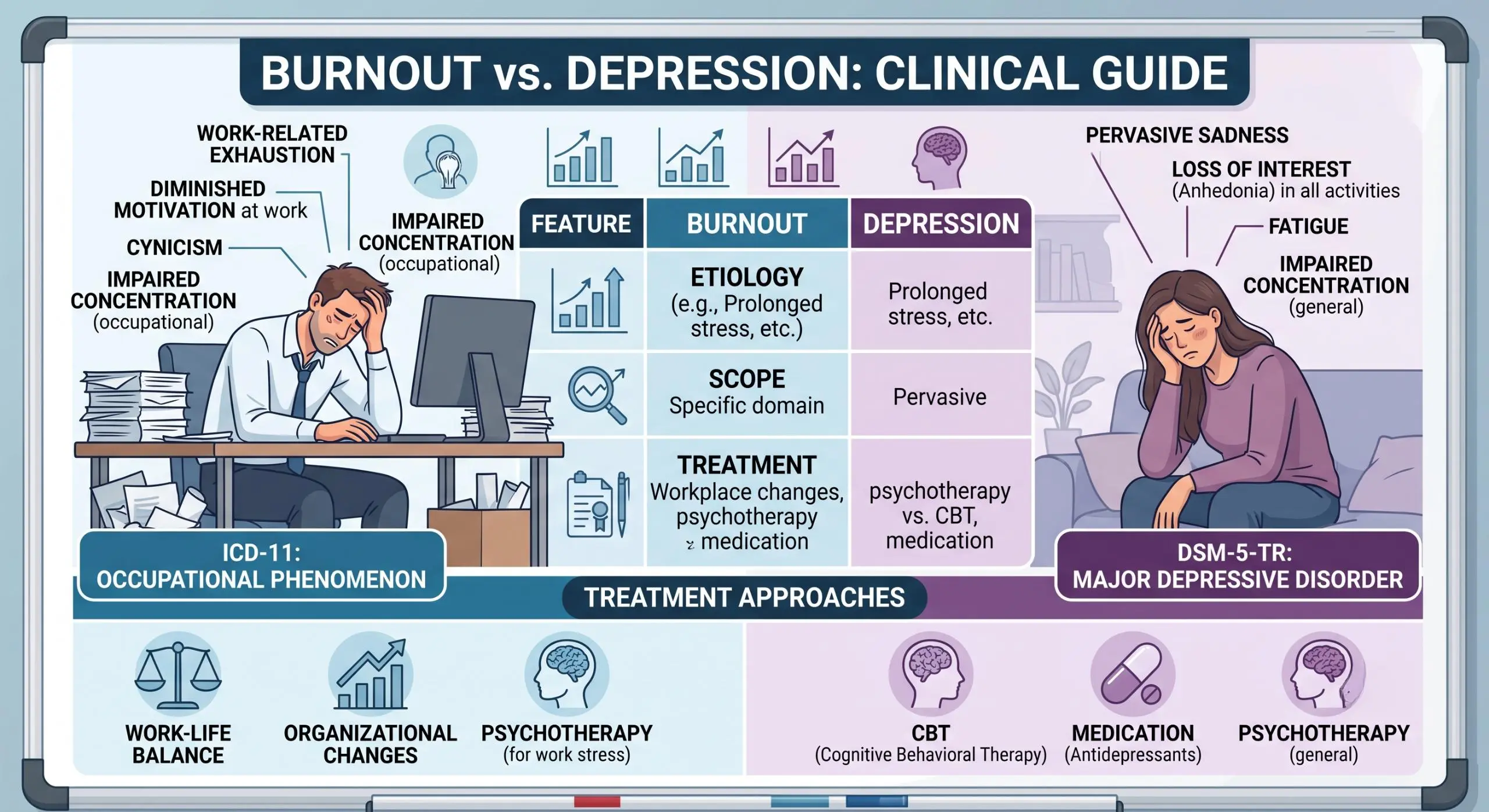
The distinction between burnout and depression represents one of the most clinically significant diagnostic challenges in contemporary mental health practice. While both conditions present with overlapping symptoms including exhaustion, impaired concentration, and diminished motivation, their etiologies, scope, and treatment responses differ fundamentally. This article provides a comprehensive clinical overview of burnout and depression, examining their definitions, diagnostic criteria, overlapping features, distinguishing characteristics, and evidence-based treatment approaches. Special attention is given to the World Health Organization’s classification of burnout as an occupational phenomenon in the ICD-11, the DSM-5-TR diagnostic criteria for major depressive disorder, and the clinical implications of their co-occurrence. By synthesizing current research and expert consensus, this guide aims to equip healthcare professionals with the tools necessary for accurate differential diagnosis and appropriate treatment planning.
1. Introduction
When patients present with complaints of persistent exhaustion, diminished motivation, and emotional detachment, clinicians face a critical diagnostic question: Is this burnout, depression, or both? The answer carries significant treatment implications, yet the symptomatic overlap between these conditions often complicates clinical assessment.
Burnout and depression share a constellation of symptoms including fatigue, cognitive impairment, and social withdrawal . However, their origins, scope, and response to intervention differ substantially. Burnout arises from chronic workplace stress that has not been successfully managed, while depression is a clinical mood disorder affecting multiple domains of functioning and often persisting without identifiable external triggers .
The clinical importance of accurate differentiation cannot be overstated. Misdiagnosing depression as burnout may delay appropriate psychiatric intervention, while misidentifying burnout as depression may lead to unnecessary pharmacotherapy while overlooking critical workplace modifications. Furthermore, prolonged burnout can increase the risk of developing clinical depression, making early recognition and intervention essential .
2. Defining Burnout: Conceptual and Diagnostic Considerations
2.1 Historical Context and Evolution
The term “burnout” was introduced in the 1970s by psychologist Herbert Freudenberger to describe a state of emotional depletion and amotivation observed in volunteers working long hours in demanding helping professions . Freudenberger identified physical manifestations including exhaustion, fatigue, and insomnia, alongside behavioral features such as irritation, frustration, and cynicism. Notably, he observed that those most susceptible were “the dedicated and the committed” individuals with “a need to give” .
The concept has historical antecedents, including the medieval notion of “acedia”—described as a state of mental and physical exhaustion accompanied by apathy and cognitive impairment. Interestingly, acedia was later merged with “tristitia” (depression) by Pope Gregory in the sixth century, perhaps initiating the historical conflation of these distinct conditions .
2.2 Current Definition and Classification
The World Health Organization (WHO) included burnout in the 11th Revision of the International Classification of Diseases (ICD-11) as an occupational phenomenon rather than a medical condition . It appears in the chapter “Factors influencing health status or contact with health services”—a section reserved for reasons people contact health services that are not classified as illnesses .
The ICD-11 defines burnout as:
“a syndrome conceptualized as resulting from chronic workplace stress that has not been successfully managed. It is characterized by three dimensions:
feelings of energy depletion or exhaustion;
increased mental distance from one’s job, or feelings of negativism or cynicism related to one’s job; and
reduced professional efficacy.”
Critically, the WHO explicitly states that “burnout refers specifically to phenomena in the occupational context and should not be applied to describe experiences in other areas of life” . This workplace-specific scope represents a fundamental distinction from depression.
The American Medical Association has emphasized that the ICD-11 definition positions burnout “primarily related to the environment, such as when there is a mismatch between the workload and the resources needed to do the work in a meaningful way” . This environmental attribution has significant implications for intervention: “The best response to burnout is to focus on fixing the workplace rather than focusing on fixing the worker” .
2.3 Diagnostic Challenges and Measurement Issues
Despite its inclusion in ICD-11, burnout presents substantial diagnostic challenges. The condition is not listed in the DSM-5-TR, and no universally accepted diagnostic criteria exist .
The Maslach Burnout Inventory (MBI) remains the most widely used measure, employed in over 90% of burnout research studies. The MBI assesses three dimensions:
Emotional exhaustion
Depersonalization (cynicism and detachment)
Reduced personal accomplishment
However, the MBI has several limitations. It was developed for human services professionals and lacks validated cut-off scores for determining “caseness.” Researchers have adopted 47 different cut-off procedures across studies, contributing to prevalence estimates ranging from 0% to 80.5%—a range that “strains credulity” according to systematic reviewers .
Other instruments have expanded the conceptualization. The Burnout Assessment Tool (BAT) includes seven scales encompassing exhaustion, mental distance, emotional impairment, cognitive impairment, depressed mood, psychological distress, and psychosomatic complaints. The Sydney Burnout Measure (SBM) similarly captures exhaustion, cognitive dysfunction, loss of empathy, withdrawal, impaired performance, and unsettled mood .
A key diagnostic challenge is that all burnout measures risk “false-positive” diagnoses, as high scores can be returned by individuals with depression, anxiety, physical conditions such as severe anemia, or those receiving chemotherapy. Consequently, clinicians should view these measures as screening strategies rather than definitive diagnostic tools .
2.4 Arguments for and Against Psychiatric Classification
The debate regarding burnout’s status as a psychiatric condition remains unresolved. Arguments against classification include the absence of consensus on intrinsic constructs, the lack of validated cut-off scores, and the normative nature of burnout experiences .
Furthermore, no burnout measure requires a minimum duration for symptom presence, raising the risk of identifying temporary exhaustion rather than a clinically significant syndrome. The ICD-11’s positioning of burnout as an “occupational phenomenon” rather than a medical condition reflects these concerns .
Proponents of recognition, however, argue that the ICD-11 provides a more detailed definition than ICD-10, potentially enabling improved data collection and understanding of causes and solutions. As the WHO noted, “Having said that, the importance of well-being in the workplace is well understood by WHO” .
3. Defining Depression: Clinical Criteria and Classification
3.1 Major Depressive Disorder: DSM-5-TR Diagnostic Criteria
In contrast to burnout, depression is a recognized mental health condition with clearly defined diagnostic criteria. According to the DSM-5-TR, a diagnosis of Major Depressive Disorder (MDD) requires the presence of five or more symptoms during the same two-week period, representing a change from previous functioning, with at least one symptom being either:
Depressed mood, or
Loss of interest or pleasure (anhedonia)
The complete symptom criteria include:
Depressed mood most of the day, nearly every day (subjective report or observation)
Markedly diminished interest or pleasure in all or almost all activities
Significant weight loss or gain (>5% body weight) or appetite change
Insomnia or hypersomnia nearly every day
Psychomotor agitation or retardation nearly every day
Fatigue or loss of energy nearly every day
Feelings of worthlessness or excessive/inappropriate guilt
Diminished ability to think or concentrate, or indecisiveness
Recurrent thoughts of death, suicidal ideation, or suicide attempt
Additional criteria require that:
Symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning
The episode is not attributable to substance effects or another medical condition
The episode is not better explained by bereavement (though prolonged grief disorder is now recognized)
3.2 Clinical Specifiers
The DSM-5-TR includes several specifiers to characterize depressive episodes more precisely:
Anxious Distress Specifier: Requires at least two symptoms including feeling keyed-up, unusually restless, difficulty concentrating due to worry, fearing something awful may happen, or worrying about losing control. High anxiety levels correlate with higher suicide risk, longer illness duration, and greater treatment nonresponse .
Melancholic Features: Requires either loss of pleasure in all activities or lack of reactivity to pleasurable stimuli, plus three of: distinct quality of depressed mood, depression worse in the morning, early morning awakening, marked psychomotor disturbance, significant anorexia/weight loss, or excessive guilt .
Atypical Features: Characterized by mood reactivity (mood brightens in response to positive events) plus at least two of: significant weight gain or increased appetite, hypersomnia, leaden paralysis, or long-standing interpersonal rejection sensitivity. Vegetative symptoms show “reversed polarity” (increased rather than decreased sleep, appetite, and weight) .
4. Burnout vs. Depression: Clinical Differentiation
4.1 Scope and Context
The most fundamental distinction lies in the scope of impairment. Burnout is contextually specific, typically linked to a particular role or situation—work, caregiving, or academic demands . Depression is pervasive, affecting multiple life domains including work, relationships, hobbies, and self-care .
As Liberty Case, MA, LPC, NCC, CCTP, explains: “Depression is a clinical condition that touches every area of life. It doesn’t clock out when you go on vacation. It affects how you sleep, eat, think, and feel about yourself and the future. And it can show up with no obvious external trigger.”
4.2 Emotional Experience
The emotional quality differs significantly:
| Feature | Burnout | Depression |
|---|---|---|
| Primary emotion | Exhaustion, cynicism, detachment | Persistent sadness, emptiness, hopelessness |
| Self-perception | “I have nothing left to give” | “I don’t feel like myself anymore” |
| Guilt/Worthlessness | Less prominent; externalizes blame | Prominent; feelings of worthlessness, excessive guilt |
| Enjoyment | May still enjoy hobbies when energy permits | Loss of interest/pleasure in previously enjoyed activities |
4.3 Response to Rest and Removal from Stressor
A key diagnostic question is whether symptoms respond to rest and removal from the stressor. “If a genuinely restful break gives you some relief, burnout is more likely,” notes Case. “If nothing moves the needle, depression deserves a closer look.”
However, clinicians should recognize that burnout recovery is not always immediate. It may take time for the mind and body to recover from chronic stress. Temporary relief during vacation with rapid symptom return upon re-exposure to the stressor is consistent with burnout . Persistent symptoms despite genuine recovery efforts suggest depression should be considered .
4.4 Symptom Overlap and Differential Features
Shared Symptoms :
Persistent fatigue or low energy
Difficulty concentrating or making decisions
Reduced motivation
Emotional withdrawal or social isolation
Feeling detached from people or activities once enjoyed
Changes in productivity or daily functioning
Sleep disturbances
Symptoms More Specific to Burnout :
Cynicism, detachment, or resentment toward work
Growing sense that efforts don’t matter
Emotional depletion rather than deep sadness
Symptoms improve when away from the stressor
May still enjoy hobbies, relationships, or downtime when energized
Symptoms More Specific to Depression :
Persistent sadness, emptiness, or hopelessness
Feelings of worthlessness, excessive guilt, or self-criticism
Loss of interest or pleasure in previously enjoyable activities
Significant changes in sleep or appetite
Slowed thinking, movement, or speech
Thoughts of death, self-harm, or suicide
4.5 Risk Factors and Vulnerability
Burnout typically results from prolonged stress with demands exceeding available resources, often accompanied by feeling underappreciated or undercompensated . Key contributing factors include:
Heavy workload and long hours
Lack of control over work
Unclear expectations
Workplace conflict
Work-life imbalance
Certain personality traits may increase burnout vulnerability, including neuroticism. A diathesis-stress model has been proposed, weighting predisposing personality styles alongside precipitating workplace factors .
Depression arises from biological, psychological, and environmental factors . Risk factors include:
Genetic predisposition
Neurochemical imbalances
Stress, loss, illness, or life changes
Prior depressive episodes
Sometimes no obvious trigger at all
4.6 Epidemiology and Prevalence
Burnout prevalence estimates remain problematic due to measurement inconsistencies. However, studies suggest approximately one-third of the workforce experiences burnout, with significantly higher rates in caring professions. One systematic review of physicians found burnout rates up to 67%, though the wide variation in measurement approaches precludes definitive conclusions .
Depression is more precisely quantified: 7.1% of US adults experienced at least one major depressive episode in 2017, with rates increasing substantially during the COVID-19 pandemic. Among physicians, 15% reported symptoms of clinical or subclinical depression .
5. The Burnout-Depression Relationship: Co-occurrence and Comorbidity
5.1 Can They Occur Together?
Yes, burnout and depression can co-occur, and chronic burnout can increase the risk of developing depression . Research published in Frontiers in Psychology indicates that prolonged burnout, when unaddressed, can spread from the original stressor into other life domains, creating conditions favorable for depressive episodes.
5.2 The Burnout→Depression Pathway
The mechanism appears multifactorial:
Chronic stress depletes physiological and psychological resources
Symptom spread from work-related to global impairment
Hopelessness about work can generalize to hopelessness about life
Social withdrawal reduces protective social support
Sleep disruption and cognitive impairment compound over time
5.3 Clinical Implications of Co-occurrence
When both conditions are present, symptoms are typically more severe and recovery more complex. Treatment must address both the external stressors contributing to burnout and the depressive symptoms requiring clinical intervention .
6. Treatment Approaches: Evidence-Based Strategies
6.1 Treating Burnout: Organizational and Individual Interventions
Organizational-Level Interventions :
Reducing workload and improving workflow efficiency
Enhancing teamwork and communication
Leadership development to support employee well-being
Ensuring adequate resources to perform job duties
Creating clear expectations and feedback mechanisms
Christine Sinsky, MD, emphasizes: “The most powerful interventions to reduce burnout are to improve workflow efficiency, teamwork and leadership” .
Individual-Level Interventions :
Taking meaningful time to rest and recover
Setting clearer boundaries around work or caregiving responsibilities
Reducing unnecessary demands where possible
Making time for restorative or enjoyable activities
Working with a therapist to address patterns contributing to burnout
Practicing mindfulness and relaxation techniques
Regular exercise and adequate sleep
Evidence for Interventions: A randomized clinical trial at Mayo Clinic tested a facilitated physician small-group curriculum incorporating mindfulness, reflection, and shared experience over 9 months. Intervention participants showed significant improvements in meaning and engagement in work, with sustained effects at 12 months .
6.2 Treating Depression: Clinical Approaches
Unlike burnout, rest alone is generally insufficient to address depression . Evidence-based treatments include:
Psychotherapy:
Cognitive Behavioral Therapy (CBT)
Interpersonal Therapy (IPT)
Other evidence-based modalities
Pharmacotherapy:
Antidepressant medications
Often combined with psychotherapy for optimal outcomes
Additional Strategies :
Sleep, exercise, and stress reduction
Social support
Lifestyle modifications
Treatment-Resistant Depression: When first-line treatments prove insufficient, additional options include transcranial magnetic stimulation (TMS) and other approaches. Importantly, treatment resistance “doesn’t mean you’ve failed treatment” .
6.3 Treating Co-occurring Burnout and Depression
When both conditions are present, treatment must address both domains simultaneously:
Working with a therapist while making workplace changes
Setting interpersonal and workplace boundaries
Developing relaxation techniques for acute stress
Implementing healthy lifestyle changes
Medication may provide symptom relief enabling meaningful therapy participation
7. Special Considerations
7.1 Burnout and Neurodivergence
Burnout can present differently in neurodivergent individuals, including those with ADHD and autism. Research suggests these groups may be at higher risk of burnout due to factors including masking, sensory overload, and navigating environments not designed for their needs. Additionally, depression and ADHD frequently co-occur, complicating symptom assessment. Clinical evaluation should consider these factors and individual needs when planning treatment .
7.2 Physician and Healthcare Professional Burnout
Healthcare professionals face particularly high burnout rates. In a 2019 report, 39% of psychiatrists and nearly 50% of physicians across multiple specialties described themselves as “burned out” . Key vulnerability areas include:
WORK Mnemonic for assessing burnout vulnerability :
Workload: Satisfaction with time for self-care, recreation, and down time
Oversight: Satisfaction with flexibility and autonomy in professional life
Reward: Perceived fairness of feedback, advancement opportunities, compensation
Kinship: Quality of cooperation, collaboration, and collegial support
Persistent dissatisfaction in any area warrants strategies to promote workplace engagement, job satisfaction, and resilience.
8. Clinical Decision-Making: When to Refer
8.1 Clinical Assessment Questions
Case recommends asking:
Are symptoms mostly tied to a specific stressor?
Do you still enjoy hobbies and relationships when you have energy for them?
Have symptoms improved after time off, rest, or stepping away from the stressor?
Do you feel persistently sad, hopeless, or worthless?
Are you experiencing symptoms of both?
8.2 When to Seek Professional Help
Consider referral or evaluation when:
Symptoms have lasted more than a few weeks
Symptoms interfere with daily functioning
Symptoms aren’t improving despite rest and recovery efforts
Suicidal thoughts are present
Depression is suspected
Start with a primary care provider or therapist: Medical evaluation can rule out physical causes while mental health assessment identifies burnout, depression, or other conditions.
Seek psychiatric evaluation when symptoms are worsening, not improving, or depression is suspected.
8.3 Red Flags Requiring Urgent Referral
Thoughts of death, self-harm, or suicide
Inability to perform basic self-care
Severe functional impairment
Psychotic symptoms
Catatonia
9. Conclusion
Burnout and depression, while sharing many symptoms, are fundamentally distinct conditions requiring different treatment approaches. Burnout is a workplace-related syndrome of exhaustion, cynicism, and reduced efficacy, classified as an occupational phenomenon in ICD-11. Depression is a pervasive mood disorder affecting all life domains, with established diagnostic criteria in the DSM-5-TR.
Accurate differentiation is clinically essential. While burnout responds to rest, boundary-setting, and workplace modifications, depression typically requires psychotherapy, pharmacotherapy, or both. When conditions co-occur, treatment must address both the external stressors and the depressive symptoms.
Clinicians should view burnout assessment tools as screening strategies rather than definitive diagnostic instruments, recognizing the risk of false-positive diagnoses. A thorough clinical evaluation, careful history-taking, and exclusion of alternative conditions are essential for accurate diagnosis.
Ultimately, whether dealing with burnout, depression, or both, effective support is available. Understanding the drivers of symptoms is the essential first step toward recovery.
10. References and Resources
Primary Sources
Parker, G., & Tavella, G. (2022). Current issues in relation to burnout’s definition, measurement, prevalence and management: A narrative review. Psychiatry Research. Elsevier. Source
Parker, G., & Tavella, G. (2022). The Diagnosis of Burnout: Some Challenges. The Journal of Nervous and Mental Disease, 210(7), 475-478. Source
ManipalCigna. Difference Between Burnout and Depression: Signs & Diagnosis. Source
Hategan, A., & Gibson, M. Physician burnout vs depression: Recognize the signs. MDEdge. Source
World Health Organization. Burn-out an “occupational phenomenon”: ICD-11 Definition. Source
American Medical Association. (2019). WHO adds burnout to ICD-11: What it means for physicians. Source
Medscape. (2019). Burnout Inclusion in ICD-11: Media Got It Wrong, WHO Says. Source
American Medical Association. (2019). WHO adds burnout to ICD-11: What it means for physicians (PDF). Source
DSM-5 Diagnostic Criteria for Major Depressive Disorder. Sohag University. Source
National Institutes of Health. Clinical Characteristics of Mood Disorders. NCBI Bookshelf. Source
NetCE. Major Depressive Disorder: DSM-5-TR Diagnostic Criteria. Source
Ochsner Health Network. (2024). Coding Tip: Major Depression. Source
Mayo Clinic News Network. (2024). Mayo Clinic Q and A: Emotional exhaustion. Source
Mayo Clinic Staff. (2023). Job burnout: How to spot it and take action. Mayo Clinic. Source
West CP, Dyrbye LN, Satele DV, Sloan JA, & Shanafelt TD. (2012). Interventions to improve physician well-being. Journal of General Internal Medicine. Stanford University. Source
Key Organizations
| Organization | Focus | Website |
|---|---|---|
| World Health Organization | ICD-11 classification | who.int |
| American Medical Association | Physician well-being resources | ama-assn.org |
| Mayo Clinic | Clinical guidance and research | mayoclinic.org |
| American Psychiatric Association | DSM-5-TR diagnostic criteria | psychiatry.org |
| National Institute of Mental Health | Depression research and resources | nimh.nih.gov |
This article is intended for healthcare professionals and provides clinical guidance for educational purposes. Clinical decisions should always consider individual patient circumstances and be made in consultation with appropriate specialists.
